
Enhancing Patient Autonomy in Rehabilitation Therapy
Enhancing Patient Autonomy in Rehabilitation Therapy
Increasing effectiveness of Rehabilitation therapy time for patients with Rheumatic & Musculoskeletal Diseases
MY ROLE
UX Designer & Researcher
TEAM
2 UX Designers | 2 UX Writers | 1 Product Manager
STAKEHOLDERS
Health Service Executive (HSE) Spark Innovation, IE
Peamount Healthcare, IE
University College Dublin, IE
National College of Art and Design, IE
PRODUCT
HealthTech Assistive Device (B2B, B2C SaaS)
TIMELINE
12 weeks
CONTRIBUTIONS
Design Lead | Primary Research, Data Analysis, Observational Study, Lo & Hi-fidelity Prototypes, User Flows, User Interviews, Service Design, UX Research
* the challenge
* the challenge
HSE Spark Innovation aimed at increasing the effectiveness of Rehabilitation therapy for patients affected with Rheumatic and musculoskeletal diseases (RMDs) at Peamount Healthcare, Dublin. Our goal was to address the issue of underutilized rehabilitation time and develop an intervention that supports patients in maximizing their rehabilitation time, to optimize recovery outcomes.
HOW MIGHT WE
enable patients to independently engage in therapy practices during their free time?
WHAT ARE THE
challenges that patients face while trying to carry out therapy practices by themselves?

* the proposed intervention
* the proposed intervention
We designed an AI-powered Interactive Rehabilitation Mirror, that assists users in independently continuing therapy through gamified activities, social collaboration and reducing stigma associated with assistive technologies.
improving patient onboarding
increasing patient autonomy

Offering real-time guidance
Jump to SEE THE FINAL DESIGN
* the impact
* the impact
The proposed assistive tool enhances patient onboarding and engagement with educational resources through accessible, inclusive design. By integrating rehabilitation activities into daily routines, it fosters motivation for independent participation.
01
enhancing patient engagement through guided onboarding
deliver structured, interactive onboarding
reduces cognitive overload
accelerates adjustment to the environment
increases motivation to engage in rehabilitation during free hours
02
improving resource accessibility
provide on-demand access to resources
support memory recall through reminders, visual prompts, and logging
reduce reliance on memory alone
increasing patient autonomy and engagement
03
integrating rehabilitation into the everyday
encouraging regular use of therapy tools without staff dependency
offering real-time guidance and feedback
normalizing practice as part of daily activity, thus building patient confidence and adherence
* the process
* the process
The team adopted a 6-step design process to address the challenge of supporting individuals in rehabilitation therapy. This allowed the team to deconstruct the research questions, overcome assumptions, and identify opportunities for potential interventions based on research findings.


discover
what are RMDs?
RMDs within global context
existing HCI literature findings
empathize
understanding the user
out-patient participant observations
affinity mapping of individual observations
in-patient participant observations
listening to the user
define
thematic analysis as a method for analysing data
re-defining the design challenge
ideate
our brainstorming & ideation process
PROTOTYPE + TEST
low-fidelity prototyping
co-design workshop
gathering feedback
evaluate
high-fidelity prototyping
evaluation
feasibility of the proposed intervention
potential future scope in design
* discover
* discover
what are RMDs?
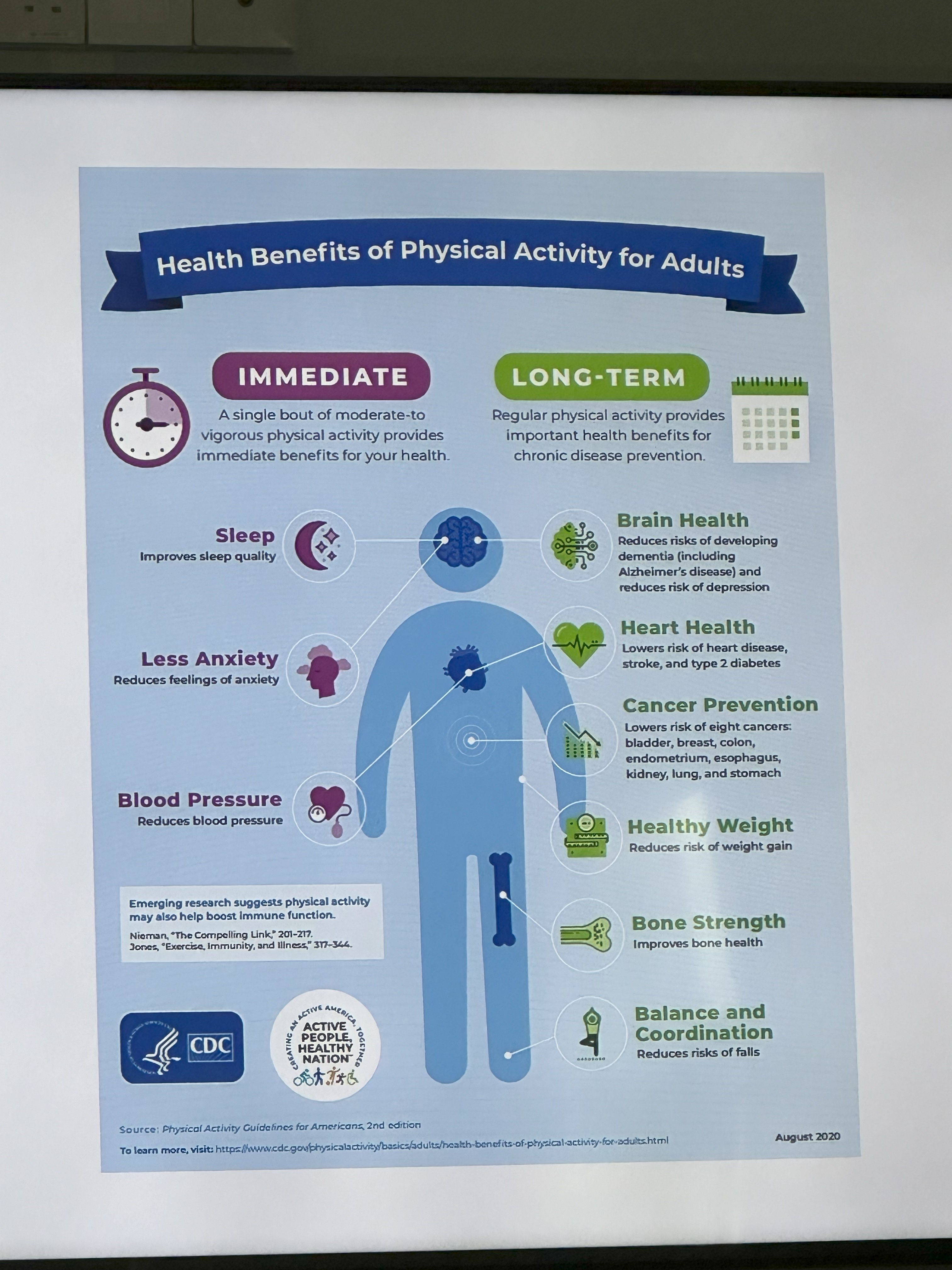
Rheumatic and musculoskeletal diseases (RMDs) are a group of chronic conditions that affect the joints, muscles, and bones. These bring about lifestyle changes, can lead to disability within 10 years of onset and can cause hindrances in everyday routines.
The project is situated in the Republic of Ireland, where RMDs are a leading cause of disability. Consistent physiotherapy is recommended for effective recovery, yet challenges such as a shortage of rheumatologists and significant economic burdens may result in patient receiving less than the recommended therapy hours.
494 million
people living with RMDs in 2020 gloablly, projected to increase by 2050 to
1060 million

1 in 4 people
across all age groups affected in Ireland and is a main cause of disability
optimize underutilized rehabilitation time
to reduce physical, psychological strains

patients get less than recommended therapy hours
due to shortage of rheumatologists and economic burdens
Our design inquiry began with a review of prior pertinent HCI research across the domains of design for
self-management to cope with lifestyle changes
inclusion of family and friends (F&F) in rehabilitation
existing healthcare technologies
barriers to assistive technology
intrinsic & extrinsic motivations
* empathize
* empathize
understanding the user | out-patient participant observations
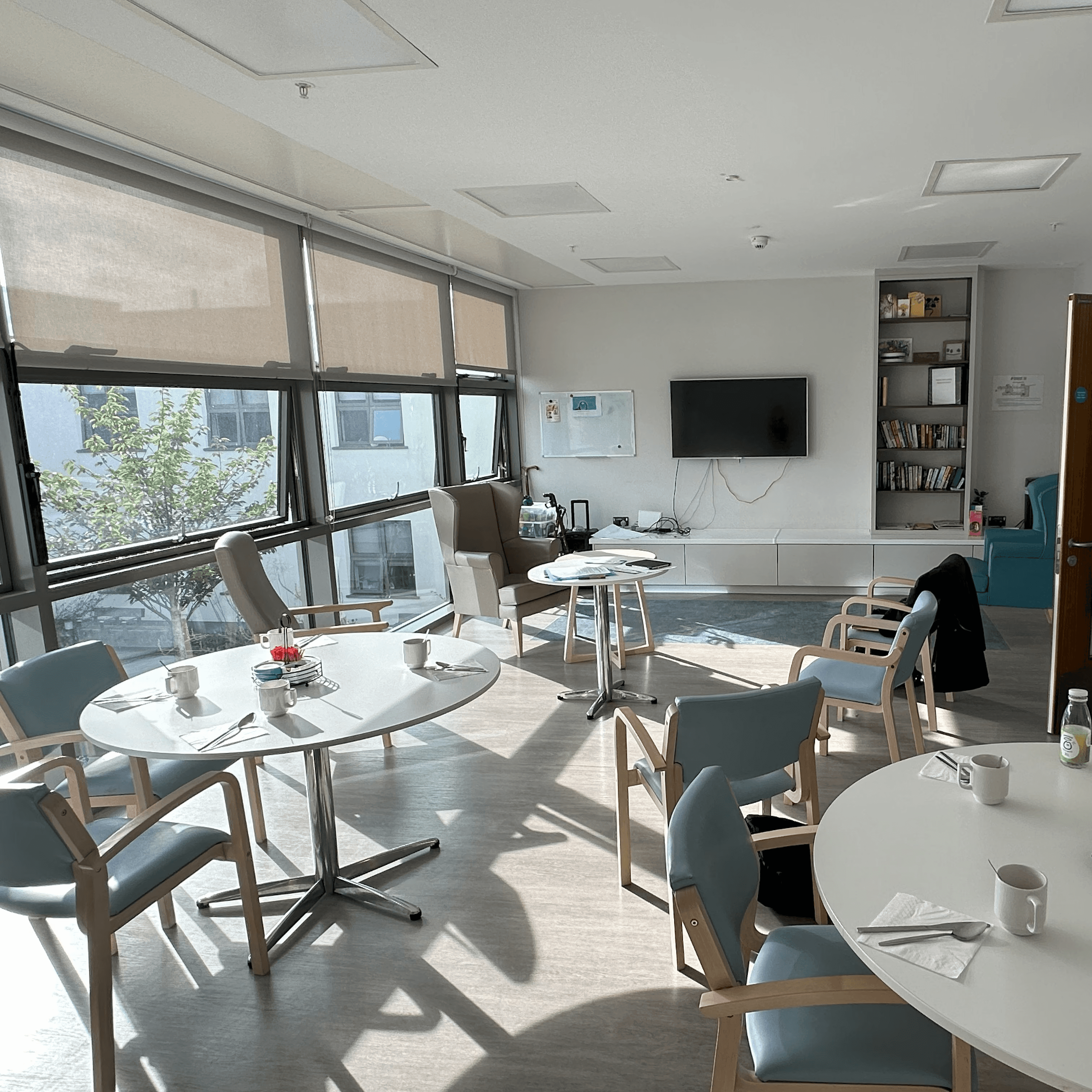
We visited the Heathcare facility on 03 separate occasions. The first visit focused on familiarizing ourselves with the facility, understanding the disease, and observing and participating in the rehabilitation program for out-patients with similar health conditions. During this initial visit, our interactions were limited to healthcare staff, which provided us with a foundational understanding of the program’s structure.

design team
healthcare staff
patients
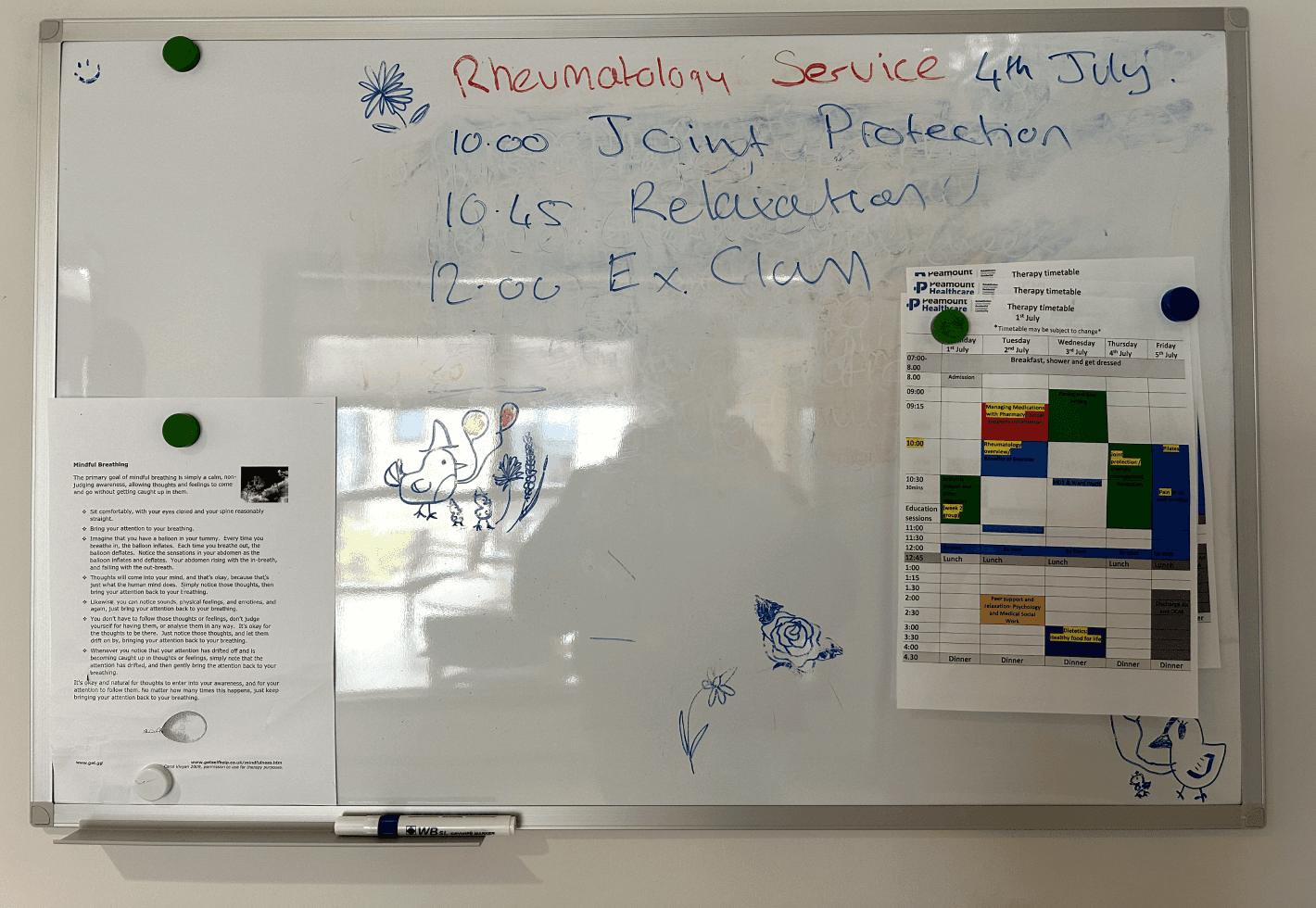
outpatient participant observations_therapy session



10:15 AM
MEETING THE STAFF
10:30 AM
exercise session
11:00 AM
educational session
12:00 PM
lunch break
12:45 PM
educational session
01:15 PM
relaxation time for patients
01:40 PM
educational session
02:15 PM
end of session
outpatient participant observations_therapy session

Homecraft key turner

ringpull can opener

reflex knife

dycem jar opener

easi-grip scissors

homecraft caring cutlery
demonstration of assistive tools by the healthcare staff



EDUCATIONAL SESSIONS, artifacts from participant observations
affinity mapping of individual observations
To ensure a comprehensive understanding of the rehabilitation activities, each member of our team actively participated and independently recorded their observations. This approach was taken to prevent any potential bias that might arise from influencing each other’s perspectives during the observation process.

field notes from participant observational study


outpatient participant observations_affinity mapping
themes identified from affinity mapping for our outpatient participant observations:
Patient Psychology | Education and Awareness | Community
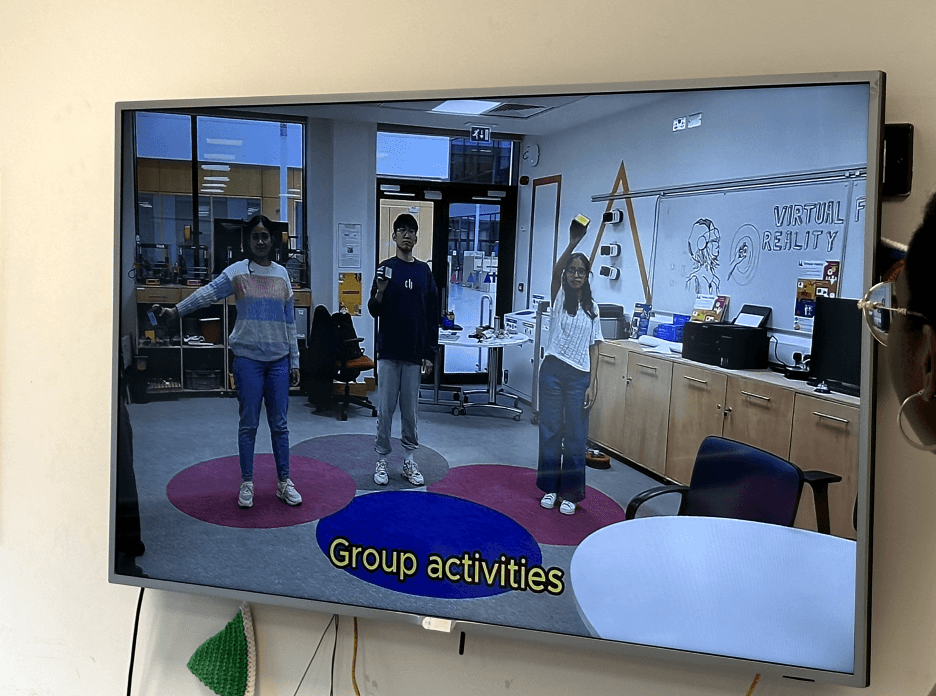
understanding the user | in-patient participant observations
We visited Peamount Healthcare to conduct another full-day participant observation, focusing on our primary target users: the inpatients. Throughout the day, we participated in all their group activities and observed them in their own environment.

individual journey map illustrating a typical day in the life of rehabilitation inpatients at Peamount Healthcare over a two-week period
Observations of inpatient behaviour, statements, and actions revealed that patients were highly willing to engage in physical activities. They actively participated in programs and engaged in meaningful discussions with their therapists, acknowledging their challenges and making efforts to address them.
listening to the user
CONDUCTING INTERVIEWS
conducted 06 semi-semi-structured interviews with healthcare professionals, occupational therapists, psychologists, and patients

The interviews revealed a complex interplay between fears, hopes, and practical challenges. Patients spoke about their anxieties regarding the loss of independence and shared their optimism and determination to achieve their rehabilitation goals, such as regaining mobility and social confidence.
Healthcare professionals offered valuable insights into their workflows and highlighted the importance of integrating technology to bridge gaps in patient care.
* define
* define
Thematic analysis as a method for analysing data
We adopted Braun and Clarke’s [2006] 06-step approach to thematic analysis particularly because it accommodates various types of qualitative data, such as observational notes, patient quotes, staff insights, and interview findings.

frequency of themes identified during interviews
The interviews reaffirmed the existing motivation and engagement levels as not being problematic for this patient group at this hospital. This raised questions about the actual barriers that prevented them from maximising their free time for engaging in rehabilitation activities. Consequently, it prompted us to rethink our problem statement and review our assumptions for the design challenge.
re-defining the design challenge
The team retraced its steps starting from week 01 to refine our project brief and research question, aiming to justify the areas of opportunity identified for potential interventions. We utilized our research findings, observational studies, readings, and interviews to support this process. This step was crucial for pinpointing the true problem areas, rather than merely continuing with those initially presented by the design partners.
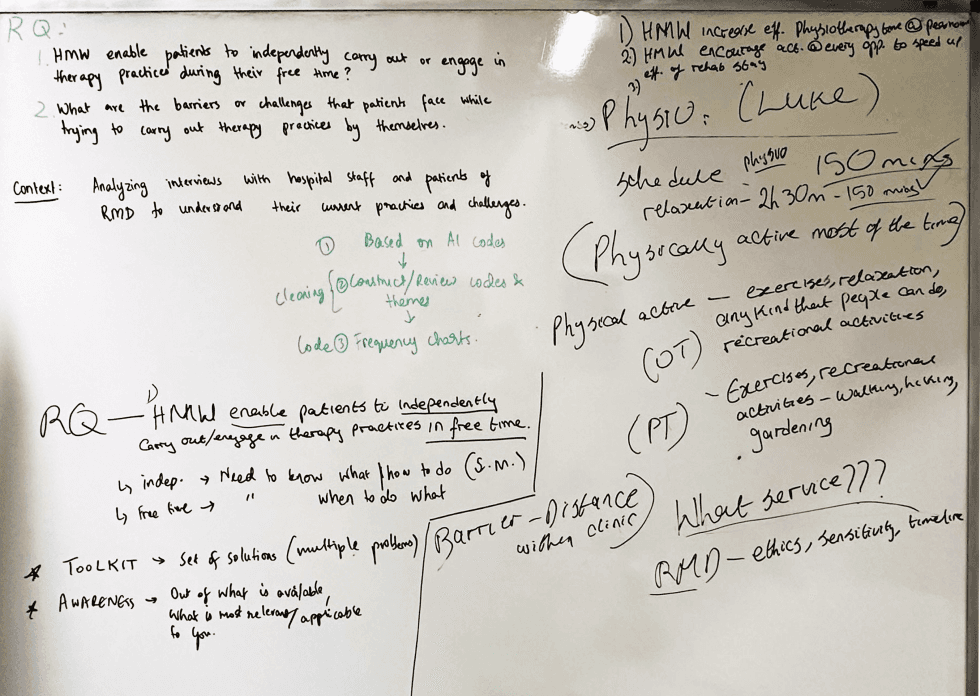
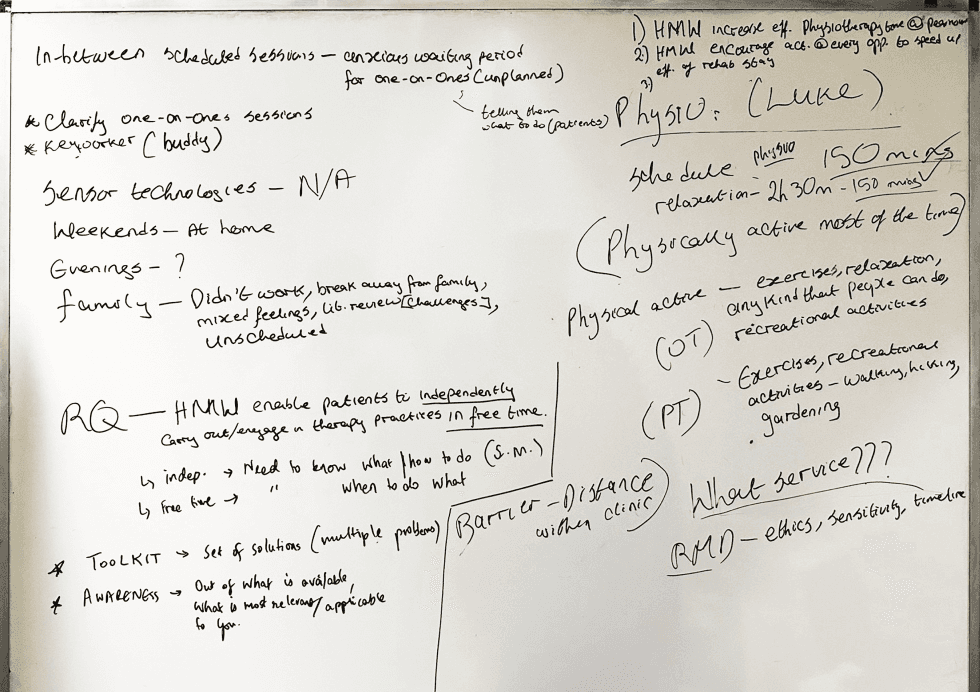
Upon reviewing the design brief and extracting insights from the thematic analysis, we identified three primary areas to focus on to enhance patient engagement in physical activities during their stay at Peamount Healthcare.
01
Optimising patient engagement through clear onboarding

02
Optimising resource accessibility and utilisation for inpatients

03
Integrating rehabilitation tools and activities into the everyday

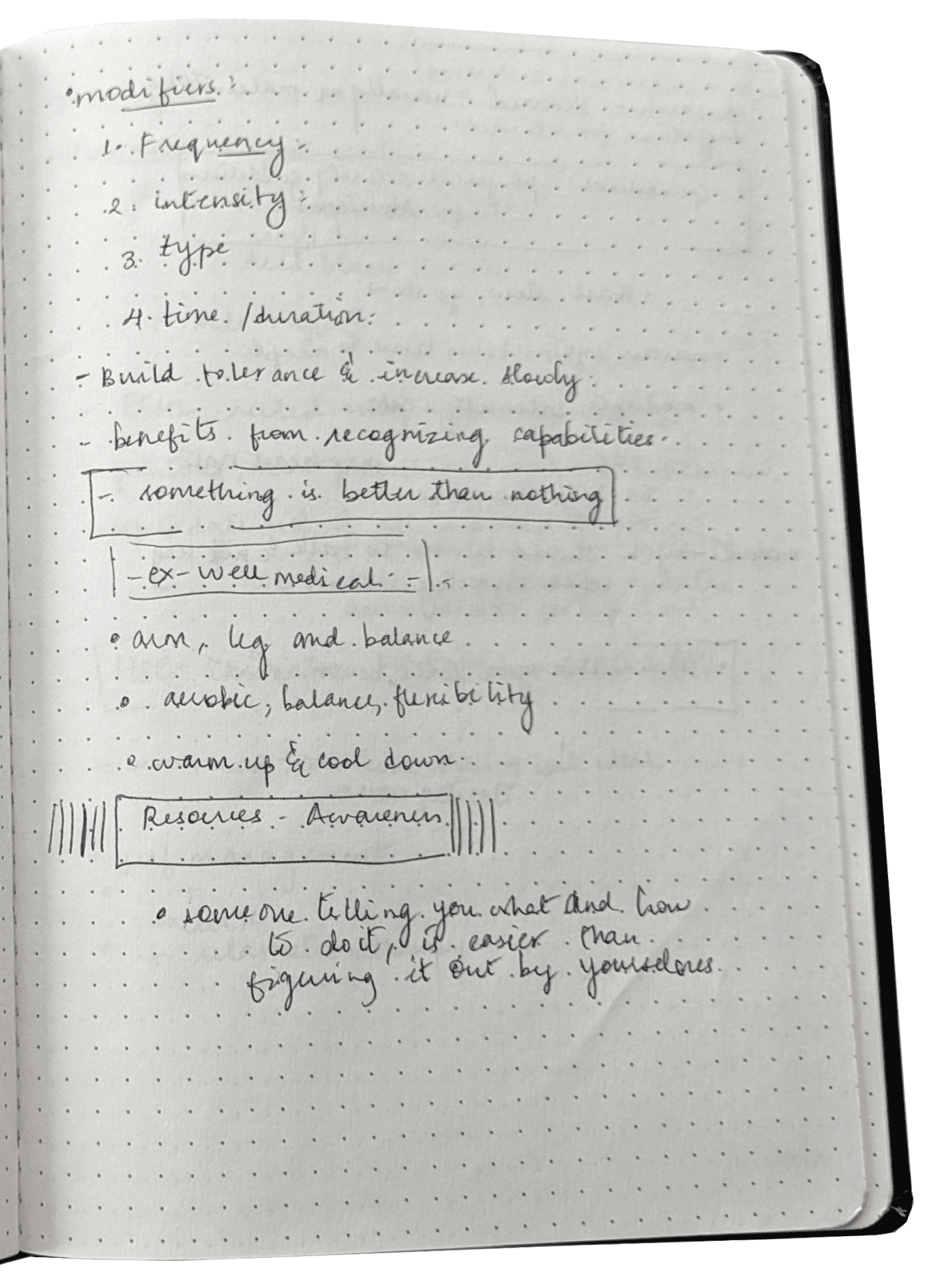
* ideate
* ideate
Our brainstorming & ideation process
The opportunity areas revealed disconnects between groups. For example, patients struggled with onboarding, affecting engagement, while healthcare providers cited the lack of digital resources as a key barrier to engagement.

Minimal reliance on strong internet connection

Accessible to different digital literacy levels
Patient inclusion in daily monitoring practices
independent of staff assistance

Prioritises information accuracy

Easy to use alongside other work
design considerations and suggestions identified from primary data collection
From these opportunity areas, we used the 10+10 design funnel method to first individually generate a diverse and creative set of ideas that captured the essence of the concept. Our ideas focused on enabling patients to engage independently in activities, while incorporating group activities to align with the community-centered design of the rehab program.

(above) concepts for_optimizing resource accessibility & utilization for inpatients
(top right) concepts for_optimising patient engagement through clear onboarding
(bottom right) concepts for_integrating rehabilitation tools & activities into the everyday




early design sketches
* prototype + test
* prototype + test
low-fidelity prototyping
At the end of the ideation phase, we selected four designs that best addressed our research question. We then created low-fidelity prototypes using materials like cardboard, foam, and paper.
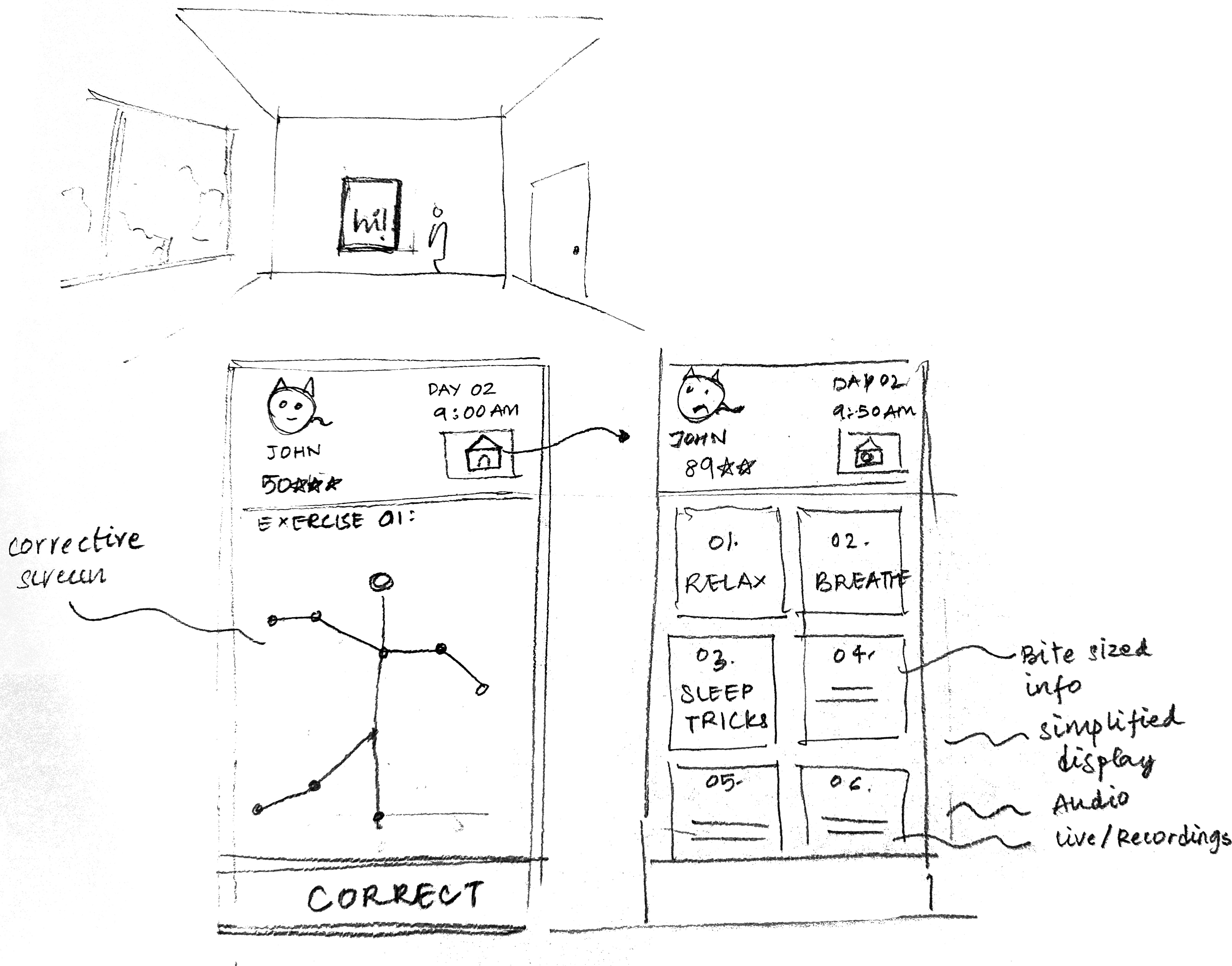
Interactive Rehabilitation Mirror
An interactive therapy mirror that transforms exercise sessions into an engaging experience.

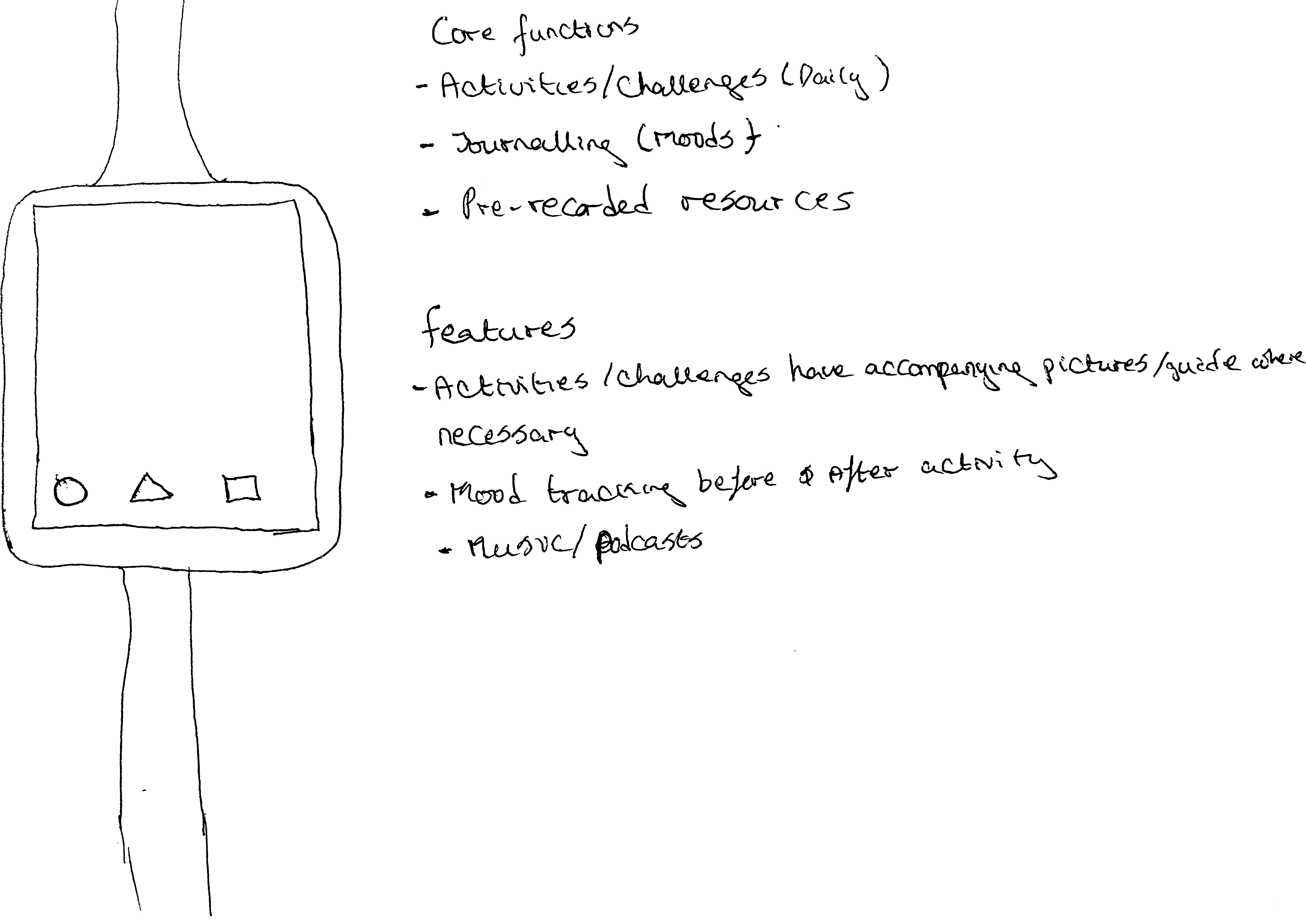
Playspace
An interactive community-building game providing engaging, bite-sized activities and real-time feedback to help its users improve mobility and strength in a fun, gamified environment.

Playspace
The “Picture Perfect” device blends into the living space as digital artwork. When interacted with, a puzzle piece flips to reveal an activity and provides guidance on-screen, integrating therapy into the daily environment.

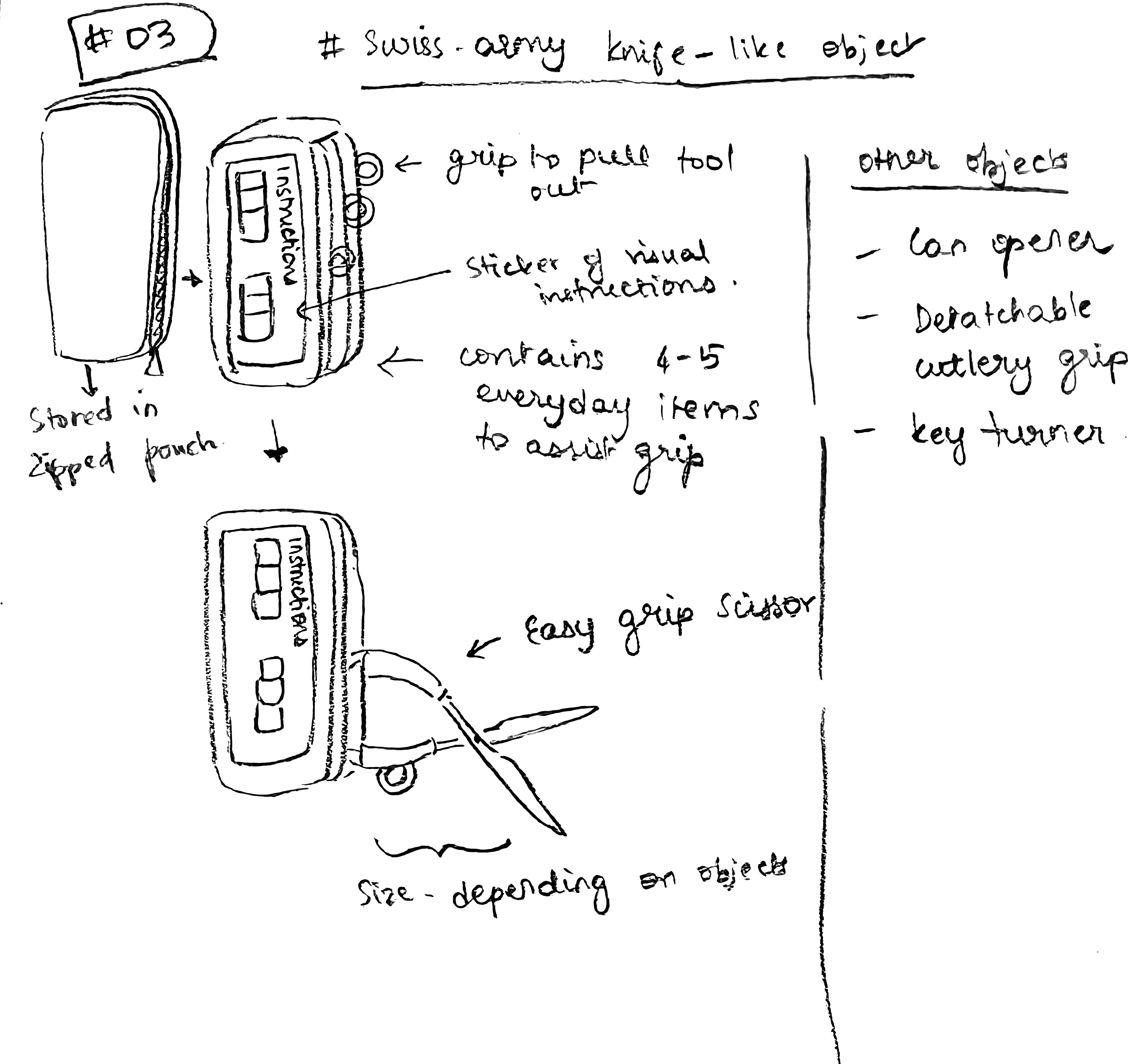
Can - Do Box
A versatile bedside companion offering a curated list of activities, including social and therapy-related options.

co-design workshop
The workshop aimed to test our design prototypes and gather participant feedback for refinement, while also expanding on or generating new ideas. By collaborating with patients, healthcare staff, and design partners, we sought to co-create practical solutions that improve independent patient engagement in rehabilitation therapy and enhance rehabilitation outcomes for rheumatology inpatients at Peamount Healthcare.
LOCATION
RMD ward living room at Peamount Healthcare
DURATION
60 minutes
PARTICIPANTS
patients : 08
therapists : 02
design partners : 03
WORKSHOP AIM
prototype presentation & evaluation
interactive brainstorming
gathering feedback


gathering feedback
We analysed the feedback the co-design workshop provided using the rating scale, feedback forms, and our notes. The rating scale was tabulated and totalled to identify the highest-scoring concept, after which we collectively reviewed the feedback forms and notes to extract recurring statements and key takeaways. Our findings highlighted key themes for suggested features and design considerations. These insights, deeply informed by the personal experiences of our stakeholders, served as the ‘building blocks’ for shaping our proposed intervention.

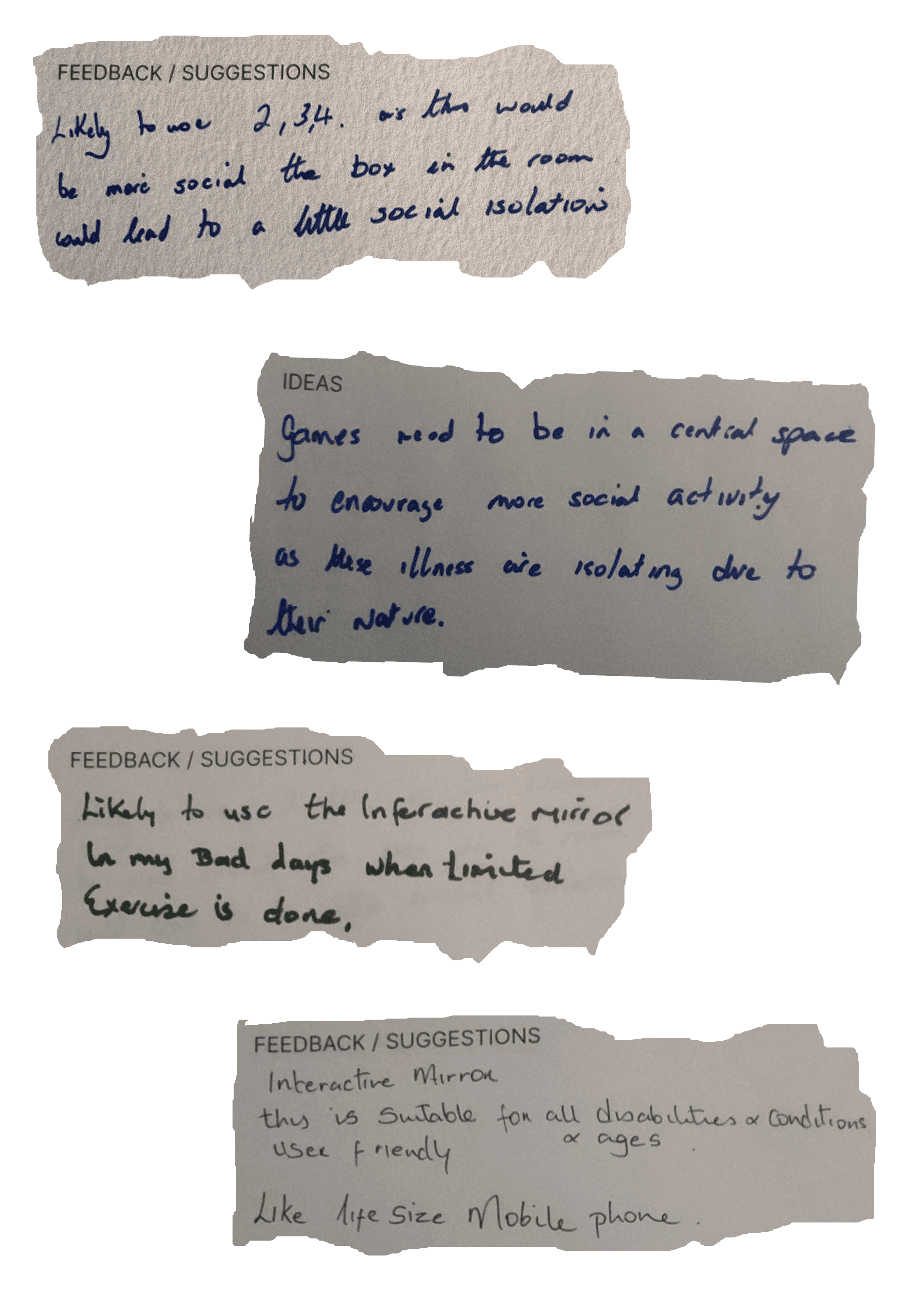
feedback from the stakeholders during the co-design workshop
01
activity and exercise encouragement
pacing support, interactive engagement, corrective guidance, real-time feedback
02
lifestyle management
self-care practices, diet and nutrition management, mental health interventions, mindfulness exercises, medication management
03
accessibility
ensure inclusivity with considerations for digital literacy, mild visual and cognitive impairments
04
environment integration
functional across different environments, from hospitals to home setting, compatible across different platforms
05
tracking
scales for tracking mood and physical state of the user
06
onboarding
educational resources provided by the hospital and instructions of how users interact with the design
07
personalisation
customise exercises based on areas of pain, fatigue levels and overall abilities
08
navigation
features to help users familiarise themselves with their surroundings effectively, digital maps or way-finding tools, alert staff when a patient needs assistance
09
inactive display
patient's schedule and reminders, visual and auditory cues, upcoming events, health tips, motivational messages
feedback from the co-design workshop
* proposed intervention + evaluate
* proposed intervention + evaluate
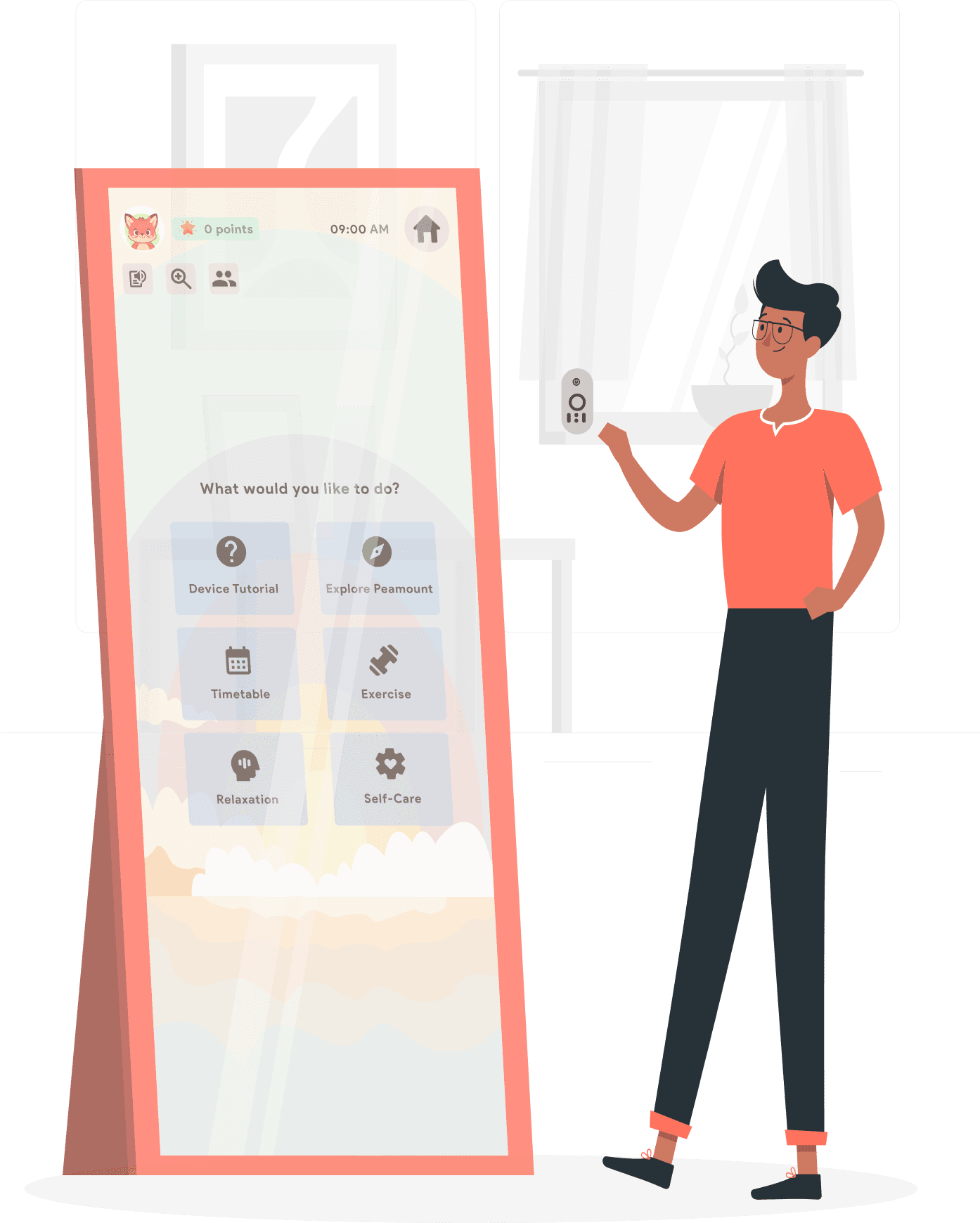
high-fidelity prototyping
The feedback from the co-design workshop revealed the interactive rehabilitation mirror as the most favoured concept, with key features like the life-size virtual coach resonating strongly with our stakeholders.
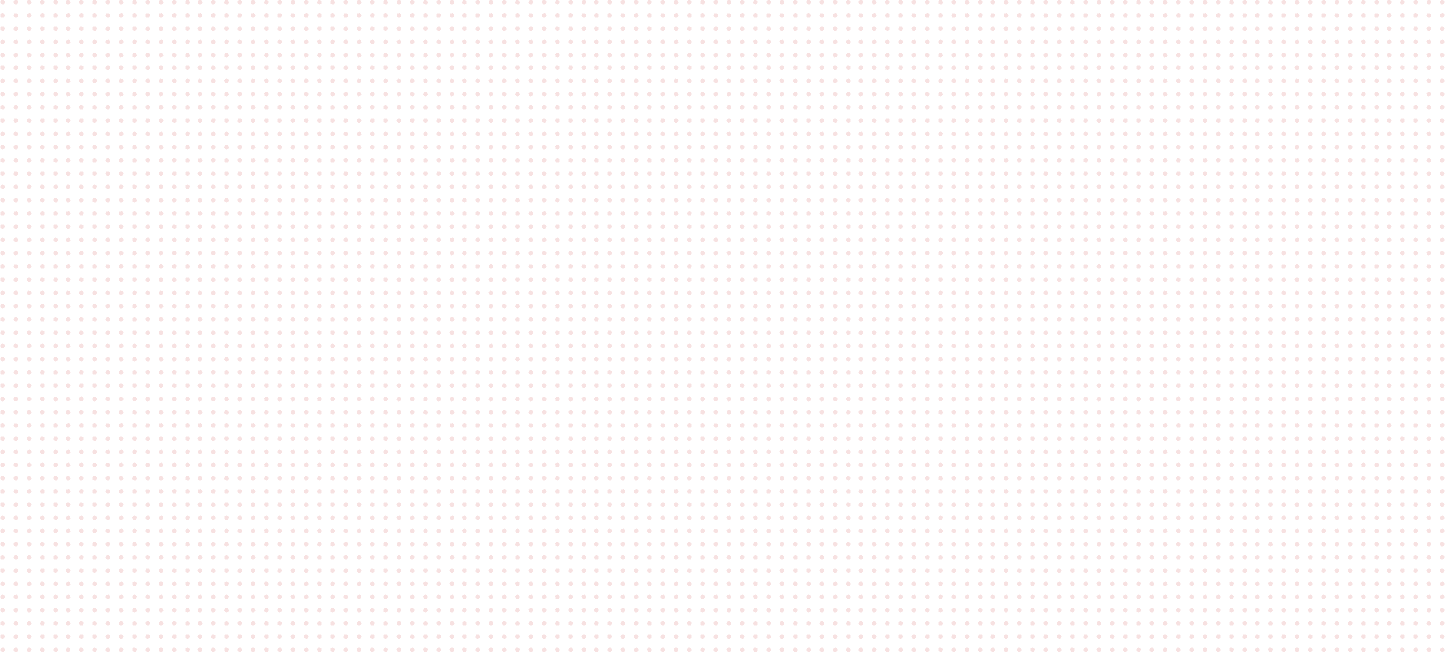
A digital mirror that helps users continue therapy in a fun and easy way during their free time. Each room is equipped with its own mirror, used individually by each patient. The mirror guides users through therapeutic activities and incorporates gamified elements to keep them motivated and engaged.
virtual coach

Resource repository

Community support

Touch, remote control
Device integration
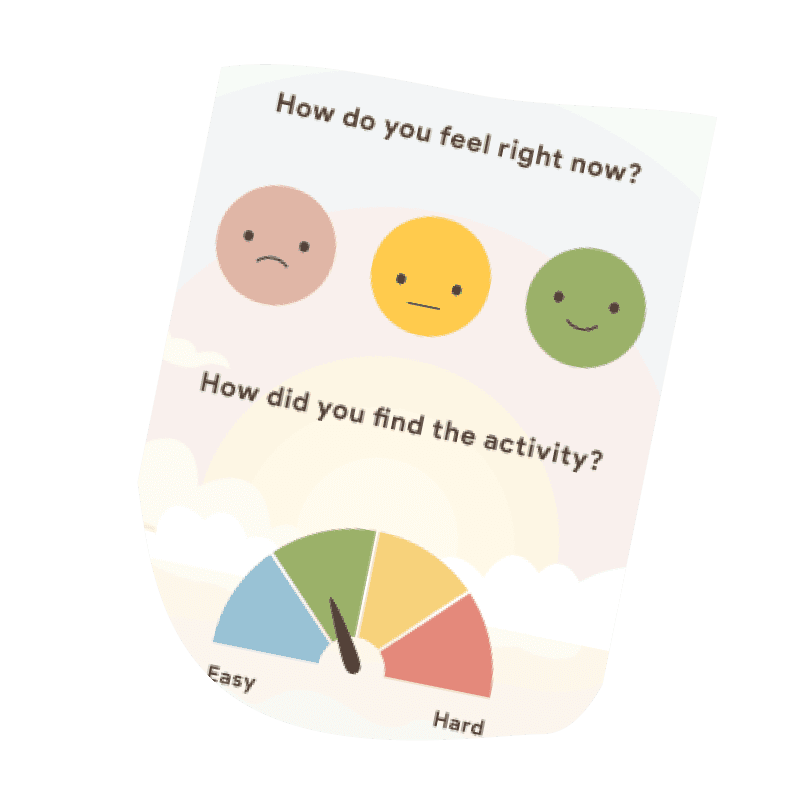
self reporting
interactive rehabilitation mirror and its key features

OVERVIEW OF THE SYSTEM ARCHITECTURE
evaluation
To evaluate user experience, usability, and areas for improvement in the hi-fi prototype, we conducted an internal evaluation using a cognitive walkthrough approach. Each participant completed specific tasks and answered a series of questions designed to guide the feedback session.
WHAT WORKED
personalized experience through AI-driven video recommendations, mood and progress tracking
clear daily schedules reduce uncertainty, self-mirroring supports posture correction
social features like "invite friends" foster motivation and shared participation
WHAT COULD BE IMPROVED
show online friends when the “Friends” icon is tapped for better social visibility
provide pre-session guidance (e.g., seating, mat) before starting videos
clarify touch vs. swipe interactions
enhance personalization with human avatars and a clear “call for help” option
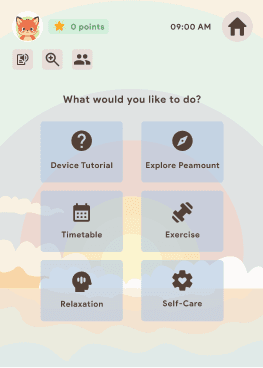
to navigate to a screen that allows you to watch a yoga video
WHAT WORKED
adjustable exercise intensity accommodates users' pain levels, mobility, and motivation
real-time recommendations support user control with options to pause, stop, or readjust
flexible pacing enhances comfort and autonomy during the rehabilitation journey
WHAT COULD BE IMPROVED
display session duration and allow speed adjustments to suit individual needs
clearly indicate mic/camera use
add an Exit button for quick session termination
offer custom music playback
include reward details, show progress
provide transparency on how user data is handled post-discharge
to navigate to a screen that guides you through some easy arm & shoulder exercises
Feasibility of the proposed intervention
a practical and achievable solution that leverages readily available components and proven technology
integrates monitoring systems, personalized recommendations based on input shared by the healthcare staff
components required are accessible, making it feasible to produce and implement
offers a practical solution to support patients in their rehabilitation journey
easy to scale and improve over time
Potential future scope in design
an app/website that patients can use to access their profile and these resources from their homes, to aid their rehabilitation progress even after they complete their program at Peamount Healthcare
a user-friendly web portal for the healthcare staff to manage recommendations for patients, and also keep record of their progress
* reflections
* reflections
learnings
01
designing for real-world complexity
The project reinforced the importance of deeply understanding user needs in complex, real-world settings - specifically in healthcare - where both patients and providers have layered, often competing, requirements.
02
value of multidisciplinary collaborations
Working with healthcare professionals, academic institutions, and innovation hubs highlighted the value of cross-functional collaboration in shaping solutions that are both research-informed and practically viable.
limitations
01
time constraints and prototype fidelity
Due to tight project timelines, there was limited scope to develop fully functional, high-fidelity prototypes. As a result, much of the testing had to rely on lower-fidelity mockups or internal walkthroughs rather than real-world interaction. This constraint limited the depth of usability testing and reduced opportunities for iterative refinement based on broader user feedback.
02
user testing opportunities
The inability to test the prototype with a broader cohort of patients and healthcare staff was a key limitation. Due to project timelines, usability evaluation was limited to internal cognitive walkthroughs, which constrained the diversity and depth of user feedback we could gather.
Back to top
I love designing.
It makes my heart go fast.
Find me here
Thank you for visiting my portfolio. Made with love and cold coffee.
Updated May 2025.
Copyright Notice
© 2025 Rutuja M. Pote. All rights reserved.
Unless otherwise stated, all content on this website - including designs, text, images, and graphics - is the intellectual property of Rutuja M Pote.
No part of this website may be reproduced, distributed, or transmitted in any form or by any means, including copying, downloading, or sharing for commercial or public use, without prior written permission from the copyright holder.